-

Boye Sokhna, Bouaré Seydou, Ky-Zerbo Odette, Rouveau Nicolas, d'Elbée Marc, Silhol Romain, Bekelynck Anne, Desclaux Alice, Larmarange Joseph and Pourette Dolorès (2020) “Challenges of HIV self-tests distribution for index testing in a context where HIV status disclosure is low: preliminary experience of the ATLAS project in Bamako, Mali” (poster), presented at the INTEREST 2020, online. http://interestworkshop.org/.Abstract: Context and Objective: In Côte d'Ivoire, Mali and Senegal, ATLAS project has introduced HIV self-testing (HIVST) as an index testing strategy, distributing HIVST kits to people living with HIV (PLHIV) during consultations for secondary distribution to their partners. Here, we present preliminary results of an ethnographic survey conducted in one HIV clinic in Bamako, Mali, where most HIV patients have not disclosed their HIV status to their partner(s), notably for women for fear of jeopardizing their relationships. In such a context, how non-disclosure affect the distribution of HIVST kits? Method: The study was conducted from September 25 to November 27, 2019, and included individual interviews with 8 health workers; 591 observations of medical consultations; and 7 observations of patient groups discussions led by peer educators. Results: Three principal barriers to HIVST distribution for index testing were identified. (1) Reluctance of PLHIV to offer HIVST to partners to whom they have not (yet) disclosed their status and desire to learn tactics for offering testing without disclosing their HIV status. (2) Near-universal hesitancy among health workers to offer HIVST to persons who, they believe, have not disclosed their HIV status to their partner(s). (3) Absence of strategies, among health workers, to support discussion of status disclosure with PLHIV. In the rare cases where HIVST was offered to a PLHIV whose partner did not know their status, either the PLHIV declined the offer or the provider left it to the patient to find a way to deliver the HIVST without disclosing his/her status. Conclusion: HIV self-testing distribution could serve as an opportunity for PLHIV to disclose their HIV status to partners. The continuing reluctance of PLHIV to heed advice to share their status and promote secondary HIV self-testing distribution highlights the structural factors (social inequalities and stigma) that limit awareness of HIV status and that favour the persistence of the epidemic. -
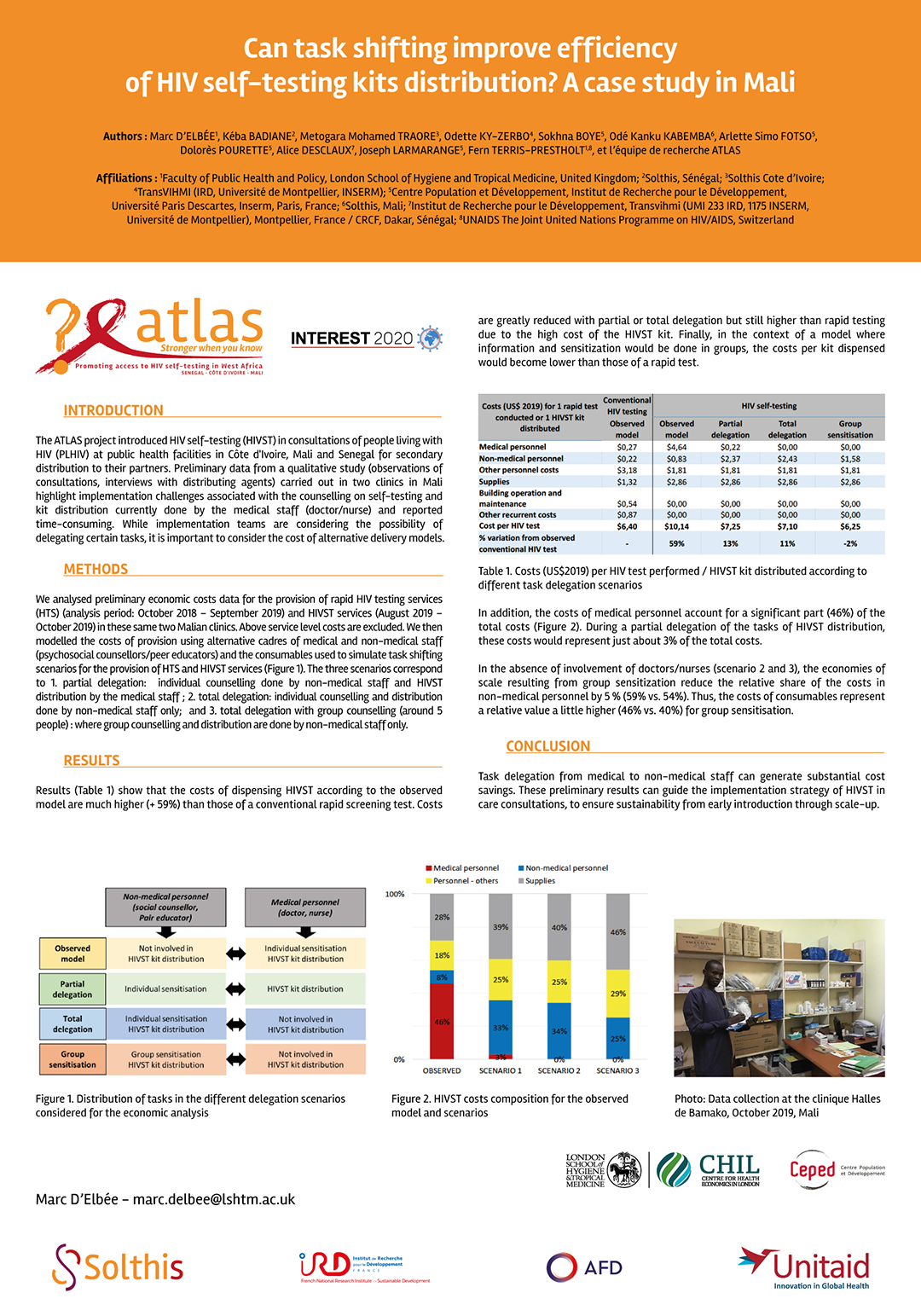
d'Elbée Marc, Badiane Kéba, Ky-Zerbo Odette, Boye Sokhna, Kanku Kabemba Odé, Traore Mohamed, Simo Fotso Arlette, Pourette Dolorès, Desclaux Alice, Larmarange Joseph and Terris-Prestholt Fern (2020) “Can task shifting improve efficiency of HIV self-testing kits distribution? A case study in Mali” (poster), presented at the INTEREST 2020, online. http://interestworkshop.org/.Abstract: Background: The ATLAS project introduced HIV self-testing (HIVST) in consultations of people living with HIV (PLHIV) at public health facilities in Côte d'Ivoire, Mali and Senegal for secondary distribution to their partners. Preliminary data from a qualitative study (observations of consultations, interviews with distributing agents) carried out in two clinics in Mali highlight implementation challenges associated with the counselling on self-testing and kit distribution currently done by the medical staff (doctor/nurse) and reported time-consuming. While implementation teams are considering the possibility of delegating certain tasks, it is important to consider the cost of alternative delivery models. Materials & Methods: We analysed preliminary economic costs data for the provision of rapid HIV testing services (HTS) (analysis period: October 2018 – September 2019) and HIVST services (August 2019 – October 2019) in these same two Malian clinics. Above service level costs are excluded. We then modelled the costs of provision using alternative cadres of medical and non-medical staff (psychosocial counsellors/peer educators) and the consumables used to simulate task shifting scenarios for the provision of HTS and HIVST services. The three scenarios correspond to 1. partial delegation: individual counselling done by non-medical staff and HIVST distribution by the medical staff ; 2. total delegation: individual counselling and distribution done by non-medical staff only; and 3. total delegation with group counselling: where group counselling and distribution are done by non-medical staff only. Results: Findings show that the unit costs per HIVST provided for the observed model are 58% higher than those of a conventional rapid test: $7,50 and $4.75, respectively. The costs are less high in scenarios of partial ($5.45, +15%) or total ($5.29, +11%) delegation but always higher than those of a rapid test due to the greater costs of consumables (HIVST kit). Finally, in the case where counselling on self-testing were carried out in a group, the costs per kit provided ($4.44, -6%) would become slightly lower than those of a rapid test, where counselling is always done individually. Conclusion: Task delegation from medical to non-medical staff can generate substantial cost savings. These preliminary results can guide the implementation strategy of HIVST in care consultations, to ensure sustainability from early introduction through scale-up. -
Ky-Zerbo Odette, Desclaux Alice, Doumenc Aïdara Clémence, Rouveau Nicolas, Boye Sokhna, Kanku Kabemba Odé, Diallo Sanata, Geoffroy Olivier, Kouadio Brou Alexis, Sow Jules Souleymane, Camara Cheick Sidi and Larmarange Joseph (2020) ““When you provide an HIV self-testing kit […] you also need to know the results”: lay providers’ concerns on HIV self-testing provision to peers, ATLAS project” (poster), presented at the INTEREST 2020, online. http://interestworkshop.org/.Abstract: Background: HIV self-testing (HIVST) is a process in which a person collects his or her own specimen (oral fluid or blood), using a simple rapid HIV test and then performs the test and interprets the result, often in a private setting, either alone or with someone he/she trusts (WHO, 2018). HIVST is convenient to reach stigmatized groups such as key populations. In the ATLAS project, provision of HIVST kits is done by lay providers to sex workers, drug users and men who have sex with men, or through secondary distribution by primary contacts to their partners and other peers. There is a shifting of paradigm because the result of an HIVST is not necessarily shared with the lay provider. How do lay providers responsible for HIVST kits distribution to key populations in West Africa adopt this new testing strategy? This abstract discusses the concerns of lay providers who offer HIVST kits to peers in the ATLAS Project (Cote d’Ivoire, Mali and Senegal). Material and Methods: We conducted seven focus group discussions with fifty-six lay providers who had experience in offering HIVST to peers (sex workers, men who have sex with men, drug users) in the three countries two months after the ATLAS project started. Results: Lay providers report no major opposition or conflict in offering HIVST kits. Testimonies from primary recipients also suggest that the HIVST was performed correctly in the case of secondary distribution. However, lay providers’ concerns remain with the lack of knowledge of the self-test results. In previous HIV testing strategies, providers usually played a key role to support their client during pre- and post-test counselling, especially when the test result was positive. Therefore, their question is how can they continue to support peers while respecting the private nature of self-testing? The concern is at two levels. At the individual level, lay providers fear that the continuum of care is not guaranteed and peers who self-test with a reactive test result may stay alone. At the collective level, lay providers fear to miss their performance objectives linked to the number of new HIV-positive cases they found and requested by some donors. Consequently, alongside HIVST provision, lay providers share their phone numbers, call back their primary recipients, or apply other indirect strategies to know the self-test result of their recipients. Conclusion: Lay providers develop strategies to learn about the issue of the HIVST they offer and to provide support to their peers following HIVST provision. Is this behaviour related to a cultural context that values social relationships or a sign of empathy to key populations and people living with HIV in a context of high stigmatization? Or is it related to existing performance objectives for new HIV-positive cases finding requested by donors? The meanings of this practice call for a deep reflection on whether or not the WHO guidelines need to be adapted to this context. -
Vautier Anthony, Rouveau Nicolas, Diallo Sanata, Traore Marinette, Geoffroy Olivier, Kanku Kabemba Odé, Doumenc Aïdara Clémence and Larmarange Joseph (2020) “Is manufacturer’s Instructions-For-Use sufficient in a multilingual and low literacy context? The example of HIV self-testing in West Africa” (poster), presented at the INTEREST 2020, online. http://interestworkshop.org/.Abstract: Background: The ATLAS project aims to promote the use of HIV self-testing (HIVST) in Côte d'Ivoire, Mali and Senegal. In order to ensure accurate HIVST use, it was necessary to evaluate if the manufacturer’s Instructions-For-Use (IFUs), standardized at the international level, provides complete, accessible and adapted information in the 3 countries’ contexts. Materials & Methods: In December 2018, cognitive interviews were conducted with 64 participants, mostly Men who have Sex with Men (40,6%) and Female Sex Workers (43,8%) in Côte d'Ivoire, Mali and Senegal. Among them, 17,2 % never performed HIV test before and 38% of participants cannot read. They were invited to perform an oral HIVST (OraQuick®) and were requested, at each step of the procedure to share their understanding of the IFU for HIVST use, of the result interpretation and of related actions to be taken. All participants had in hands the manufacturer's IFUs in French, including the free national hotline number. Half of them additionally received manufacturer's demonstration video translated into local languages. Directive interviews guide included 50 questions to collect participants’ perception of what was missing or unclear in the supporting tools. The methodology was validated with all national AIDS programmes and ministries of health. Results: Out of 64 HIVST performed, 5 results were positive (7,8%) and confirmed with additional tests. Overall, the IFU was well understood: 58 participants (92%) were able to interpret their HIVST result correctly without assistance. However, some misuses were observed at various stages, particularly for people who cannot read, with some instructions misunderstood or perceived as not adapted. Only participants who can read have access to information as “do not eat” or “do not use the test if you are on ART” as it is not illustrated in the IFUs. Most of the participants did not spontaneously identify the promotion of the free hotline number and/or the link to the demonstration video. Some procedure’s steps were misinterpreted: 7 participants (11%) did not swab correctly the flat pad along the gum, 3 participants (5%) have read the result at inaccurate time (at 20 seconds, at 5 minutes or after 40 minutes), 13 participants (20%) did not put the stand (for the tube including the liquid) in the right way and 8 other participants struggled to slide tube into the stand. Among 42 participants who can not read and/or who had not seen the video beforehand, 14 of them (33%) had at least one difficulty to interpret the result or to understand what to do after the test/result. On the other hand, the results of the cognitive interviews showed that demonstration video provides a real added value to the user’s understanding and accurate HIVST use (31 participants out of 32 found it very easy to understand with 9 of them who felt they do not need the IFUs if they previously watched the demonstration video). The video translation into local languages, produced by the ATLAS project, was very much appreciated by the participants. Conclusion: The manufacturer's IFUs alone appear not to be sufficient in a multilingual, low-literacy context to ensure accurate HIVST use. Access to additional supporting tools (complementary leaflet, demonstration video or free hotline) is essential in the 3 countries’ contexts.